
The recent announcement from the White House confirming President Donald Trump’s diagnosis of chronic venous insufficiency (CVI) has thrust this common vascular condition into the public eye. At 79, President Trump observed mild swelling in his lower legs, prompting a comprehensive medical evaluation that included bilateral lower extremity venous Doppler ultrasounds. The results confirmed CVI—a “benign and common condition, particularly in individuals over the age of 70,” according to his physician, Capt. Sean Barbabella. While the diagnosis sparked media speculation, it also provides a critical opportunity to demystify a condition affecting millions globally. CVI is not life-threatening, but its impact on quality of life and potential complications demand attention and understanding.
Section 1: Decoding Chronic Venous Insufficiency
The Mechanics of a Failing System
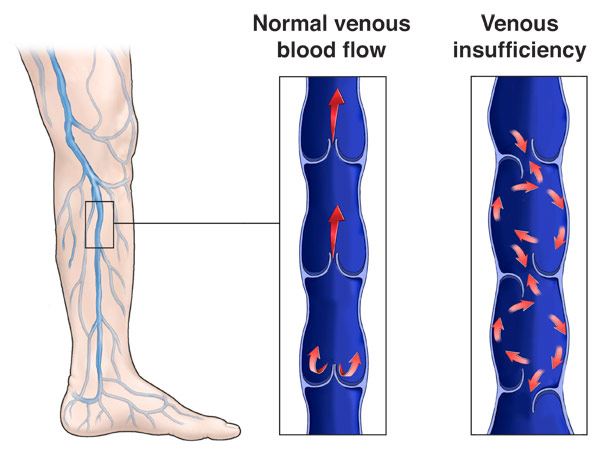
Chronic venous insufficiency arises from a fundamental breakdown in the circulatory system of the legs. Healthy leg veins rely on one-way valves and the “calf muscle pump” (often called the “second heart”) to push blood upward against gravity. When these valves become damaged or weakened, blood refluxes backward, pooling in the lower extremities. This leads to venous hypertension—chronically elevated pressure in the veins—which triggers inflammation, tissue damage, and the classic symptoms of CVI: swelling, pain, skin changes, and in advanced stages, ulcers.
Why Trump’s Diagnosis is Not Uncommon
President Trump’s age (79) places him squarely in the highest-risk demographic. Studies indicate that CVI affects approximately 1 in 20 adults, with prevalence soaring to 20–40% in those over 70. Other risk factors include obesity, prolonged standing/sitting, pregnancy, deep vein thrombosis (DVT) history, and genetic predisposition. The White House confirmed Trump had no history of DVT or arterial disease, suggesting his CVI is likely primary—stemming from age-related venous wall and valve degeneration rather than prior clotting events.
The Significance of the CEAP Classification
CVI severity is categorized using the Clinical-Etiological-Anatomical-Pathophysiological (CEAP) system:
Table: CEAP Classification Stages for Venous Disorders
| Stage | Clinical Signs | Description |
|---|---|---|
| C0 | None | Symptoms (aching, tiredness) may exist without visible signs. |
| C1 | Spider/reticular veins | Cosmetic concerns; no major functional impairment. |
| C2 | Varicose veins (>3mm) | Visible, bulging veins; may cause discomfort. |
| C3 | Edema (swelling) | Fluid accumulation, often in ankles/feet (President Trump’s current stage). |
| C4 | Skin changes | Hyperpigmentation (reddish-brown), eczema, lipodermatosclerosis (hardened skin). |
| C5 | Healed venous ulcer | Evidence of past ulceration. |
| C6 | Active venous ulcer | Open wound, typically near the ankle. |
The White House explicitly noted Trump has no skin changes (C4) or ulcers (C5/C6), placing him at stage C3—focused on swelling management.
Section 2: Symptoms, Diagnosis, and Why Trump’s Case Matters
Beyond Swollen Ankles: The Symptom Spectrum
CVI manifests progressively:
- Early Stages: Leg heaviness, aching (worse after standing), swelling (edema), restless legs, and telangiectasias (spider veins).
- Advanced Stages: Skin hyperpigmentation (hemosiderin staining), leathery texture (lipodermatosclerosis), itching (venous eczema), and finally, venous ulcers (C6).
President Trump’s reported symptoms—mild lower leg edema without pain or skin damage—align with early-to-moderate CVI. His physician emphasized he feels “no discomfort.”
Diagnostic Pathways: From Ultrasound to Differential Diagnosis
Trump’s evaluation highlights standard diagnostic protocols:
- Physical Exam: Assessment of swelling, skin integrity, and pulses (ruling out arterial disease).
- Doppler Ultrasound: Gold standard for visualizing blood flow, valve incompetence, and reflux; ruled out DVT in Trump’s case.
- Additional Tests: Echocardiogram (confirmed normal heart function), blood tests (excluded renal/kidney issues).Notably, obesity can complicate ultrasound imaging due to tissue depth, but Trump’s tests were conclusive.
Addressing the Bruises: Aspirin and Handshakes
Separate from CVI, Trump’s hand bruising was attributed to “minor soft tissue irritation” from frequent handshaking combined with daily low-dose aspirin—a common cardiovascular preventive measure that reduces blood clotting.
Section 3: Modern Management – From Compression to Cutting-Edge Procedures
Conservative Care: The First Line of Defense
Initial treatment focuses on reducing venous pressure and symptoms:
- Compression Therapy: Graduated stockings (20–30 mmHg for mild CVI; 30–40 mmHg for ulcers) improve circulation. Compliance is challenging but critical.
- Lifestyle Interventions: Weight management, walking (activates calf muscle pump), leg elevation (30 mins, 3x/day), avoiding prolonged sitting/standing.
- Pharmacotherapy: Aspirin (for anti-platelet effects), horse chestnut seed extract, or micronized purified flavonoid fraction (MPFF) to reduce edema and pain.
When Conservative Measures Fail: Medical Interventions
For persistent symptoms (like progressive swelling):
- Sclerotherapy: Foam/liquid injections collapse small varicose/spider veins.
- Endovenous Ablation: Minimally invasive procedures using radiofrequency (RFA) or laser (EVLA) energy to thermally seal malfunctioning saphenous veins.
- Combined Approaches: For complex cases (e.g., obesity), hybrid techniques like RFA + concurrent sclerotherapy improve outcomes and reduce recurrence.
Table: Advanced Treatment Options for CVI
| Treatment | Best For | Recovery | Key Advantage |
|---|---|---|---|
| Radiofrequency Ablation (RFA) | GSV reflux >5mm | 1–2 days | High success (>95%), local anesthesia |
| Endovenous Laser (EVLA) | Straight saphenous veins | 1–3 days | Low complication rate |
| Foam Sclerotherapy | Reticular veins, branches | Immediate | No anesthesia, office-based |
| Venous Valvuloplasty | Deep valve failure (rare) | Weeks | Repairs damaged valves |
Surgical Options (Severe Cases Only):
- Phlebectomy: Physical removal of varicose veins.
- Vein Bypass/Transplant: For deep venous obstruction.
Section 4: Prognosis, Prevention, and the Bigger Picture
Why Early Intervention Matters
Untreated CVI is progressive. Stage C3 edema can advance to skin breakdown (C4) and ulcers (C6), which are painful, prone to infection, and reduce mobility. Studies show ulcer recurrence rates reach 40% without proper management. Trump’s proactive approach—seeking evaluation for mild swelling—exemplifies how early diagnosis limits progression.
Obesity, Age, and Other Risk Factors
Obesity (BMI >30) increases abdominal pressure, impairing venous return. Age-related loss of vein wall elasticity also contributes. Trump’s physician highlighted weight management as part of his cardiovascular prevention regimen, indirectly supporting CVI care.
Living with CVI: Long-Term Outlook
CVI cannot be “cured,” but it can be effectively managed. With compression, exercise, and weight control, most patients maintain active lives. For President Trump, continued use of compression stockings during long periods of standing (e.g., rallies) and routine ultrasounds will be key.
Section 5: Lessons from the White House – Transparency and Awareness
Why Trump’s Disclosure is Significant
The White House’s detailed memo—addressing both leg swelling and hand bruising—sets a precedent for transparency. CVI affects ~40% of people over 70, yet remains under-discussed. Public figures normalizing such conditions reduce stigma and encourage others to seek care.
Dispelling Myths Around CVI
- Myth 1: “Swollen ankles = heart failure.” While heart/kidney issues can cause edema, CVI is a distinct (and common) vascular cause.
- Myth 2: “Vein procedures are dangerous.” Modern ablation techniques boast >95% success rates with minimal downtime.
- Myth 3: “Only women get varicose veins.” Men represent 30–45% of CVI cases.
Conclusion: A Condition Managed, Not Feared
President Trump’s diagnosis of chronic venous insufficiency is neither a political crisis nor a health catastrophe. It is a manageable condition affecting millions, particularly older adults. His case underscores critical lessons: heed early signs like swelling, prioritize non-invasive therapies (compression, exercise), and leverage modern procedures when needed. For the public, it’s a reminder that vein health is integral to overall wellness—worthy of attention, not alarm. With proactive care, individuals with CVI can lead unrestricted, active lives, embodying resilience far beyond any headline.